Research carried out by the European Centre had already shown pervasive inequalities in access to care as well as in the coverage of health insurance and potential remedies. The Covid-19 crisis brings the evidence to the headlines of the news that social inequalities and the dismantling of health and social welfare systems are killing people. The current crisis also shows that health and social care are not a ‘product’ which can be produced low-cost and provided to those with sufficiently large incomes only.
Yet, inequalities persist. While many of us continue to work in secure home offices, a great number of people have to keep working to provide our basic necessities including water, energy supply, waste collection, pharmaceuticals, groceries, and health care. Older people and persons with disabilities, in particular those living in isolation or in care homes, have complex care and support needs and were already disadvantaged before the pandemic, now they are additionally confronted with triage mechanisms and even total neglect as social services are suspended. Professionals in health and social care have struggled with working conditions already before the crisis. Now they are facing Covid-19 and a high risk exposure to the disease while many still try to maintain operating levels of standard care services. Moreover, inequalities and inequities in health care systems, in social determinants of health and in access to health care mean that those who are already disadvantaged are less equipped to deal with the virus itself – and some countries are better prepared to protect their citizens than others. It does not help to blame decisions made in the past, but we should learn from the damage done. If we really strive “to leave no one behind” we need to address Covid-19 and its consequences as a global challenge with global policies. This can be illustrated by a brief example that is much discussed in the context of Covid-19.
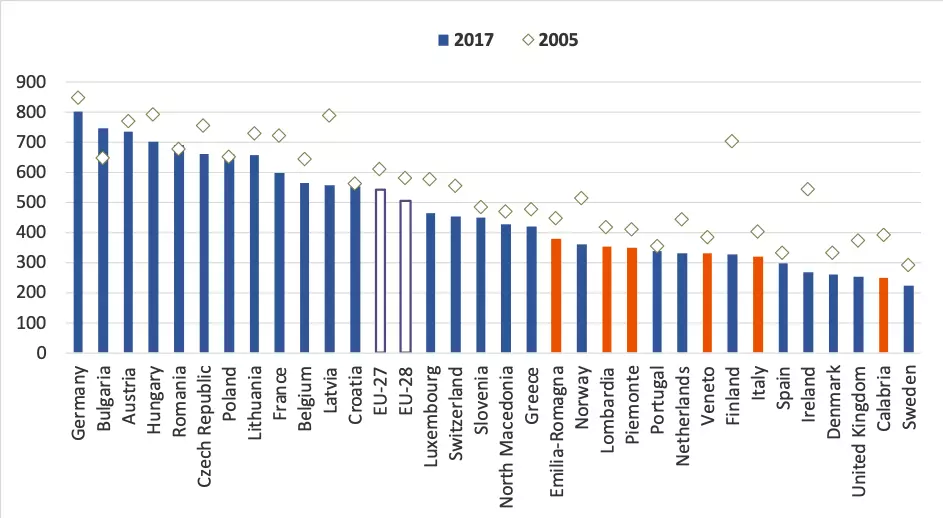
A key argument for implementing drastic measures to flatten the curve of new infections has been to avoid the breakdown of the hospital system in any affected region. All of us have seen the ‘red line’ in simulations marking the health care system capacity, i.e. the number of very sick people that can be treated in hospitals. Of course, no health system in the world is designed to have enough beds to counter the unprecedented Covid-19 emergency. However, the ‘red line’, i.e. the number of beds in hospitals, has been lowered over the past decades in all countries due to budget cuts, alleged efficiency gains and market-oriented governance. To a certain degree it is certainly recommended to reduce the role of hospitals, if countries invest in alternative care pathways such as primary care centres or long-term care in the community. However, many regions were not able to do this second step after reducing hospital beds. In this context, quantity of beds in itself is certainly not the most robust indicator – without infrastructure, sufficient staff and technical devices at disposal, a ‘hospital bed’ is nothing more than a piece of furniture. And yet, reality has shown in many regions that the ‘red line’ of hospital capacities has been exceeded rather quickly. The figure below shows the extent of reductions in hospital beds as of 2017 (latest available data) highlighting Italy and some of its regions. While hospital capacity had already been reduced before 2005, further reductions could be observed over the past years (e.g. Italy). This has made it so difficult to respond to the Covid-19 outbreak in the relatively wealthy northern regions of Italy (Lombardia, Veneto, marked in orange) with particularly hard and deadly consequences. Not only Italian authorities are worried about a potential spreading in the southern regions (e.g. Calabria), where cuts in health care infrastructure, starting from a weaker baseline, have been even stronger. The consequences of comparable imbalances between regions and countries regarding the allocation of resources to health care can also be observed in Spain and the UK, and other countries and regions are likely to experience similar impact.
These regional differences point to the necessity of European or even global strategies of cooperation also in health and social care. Rather than leaving individual regions alone to tackle the Covid-19 crisis and to compete for ventilators, masks and protective gear, we need exchange and coordination of knowledge, professionals and material across Europe and beyond. This is even more important with a view to potential learnings after the crisis to which we shall contribute with further research: