30 years ago, Austrian society made a lucky finding. Shortly before, the long-term care allowance scheme had been introduced and a few years earlier the borders to neighbouring countries had eventually become permeable. Only fifty kilometers away from Vienna or Graz, for instance, people were looking forward to a better future, but were currently unemployed or badly paid in insecure jobs. Many of them even spoke German and used the opportunity to become hired as personal assistants by Austrian families with an older person in need of care, or also directly by an adult with a disability at working age. Employment was unbureaucratic but undeclared and in any case far from real legality. This do-it-yourself care model was also discovered by those who needed to look after older family members who needed care and had space for a carer. 24-hour care was born.
The current debates about 24-hour care make me think about how Ljiljana (name pseudonymised) is doing. She comes from eastern Slovakia and when we interviewed her 10 years ago as part of a study on ‘Good care from the perspective of employees’ (Leichsenring et al., 2015; Schulmann et al., 2016), she was in her late forties, divorced, and her daughter needed financial support for her studies. Her own parents were already retired. She had given up her job as a teacher with a university degree in German and started working in 24-hour care in Austria because this had been regulated as “legal work” since 2007. She had registered as a ‘personal carer’ with the Austrian Chamber of Commerce in 2010. The income was quite attractive compared to the teacher’s salary in Slovakia, especially since two weeks of work around the clock came with two weeks of free time at home. However, Ljiljana already reported back then that her situation was being exploited. Many of her colleagues, with whom she spent the long hours in the shared taxi, were also convinced that the pay was simply too low in relation to the work done. Most recently, Ljiljana was placed with an 85-year-old client with dementia, without preparation or support. The only thing the agency gave her as a support was a manual on the subject. In fact, she is supposed to work self-employed and ‘independently’. However, in practice she is facing several dependencies. First, there is the placement agency that is brokering matching clients, and Ljiljana can hardly decline their proposals as this might lead to times without income. Secondly, she said that “it’s always a lottery as to which family constellation you’re thrown into...”.
Although it has been pointed out for years that 24-hour care, which is problematic in many respects, is a model with an expiry date, it has been further developed in Austria as an essential pillar of the local care system since its ‘legalization’ (2007). At that time, the “Home Assistance Act” was passed, which sets the minimum legal standard and is considered unique in Europe (Winkelmann et al., 2015). In Germany, Italy and Spain, personal care by migrants from Poland, Romania or South America still takes place in a largely unregulated grey area, sometimes registered or simply as undeclared work (León, 2010; Casanova et al., 2020). The Home Assistance Act was given an unfortunate title that actually points to the complexity involved in controlling the care and assistance of “people in their private households”. It is interesting to note that the employment model provided for in the law with working time regulations in accordance with the Domestic Helpers and Domestic Workers Act was only implemented in very few cases. Instead, more than 99.8% of all personal carers (around 95% are female) have chosen the self-employment alternative that was also defined in this Act. As self-employed personal carers they are not subject to any working time regulations. They are registered with the Austrian Chamber of Commerce, together with the approximately 900 placement agencies on whose services they rely and for which they also have to pay corresponding contributions. In addition, subsidies have been introduced at the federal level and in selected regions. These are granted up to a certain income limit of beneficiaries in order to compensate for the additional costs of social insurance contributions.
On the basis of these regulations, personal care became a successful model against undeclared work in this sector and a steady growth market.
The number of active personal carers rose from around 24,000 to around 63,000 between 2008 and 2019, who look after around 6% of beneficiaries receiving the long-term care allowance. The number of recipients of subsidies for 24-hour care reached their peak in 2017 at over 25,000 (BMSGPK, 2023). At this point, however, the carers from Romania had begun to overtake those from Slovakia in proportion, which meant that the original 14-day rotation of personal carers was often replaced by a monthly or even three-monthly shift of carers per client.
Overall, 24-hour care was and continues to be praised as a win-win model for everyone involved. However, the pandemic also made the fragility of 24-hour care visible (Kadi et al., 2023; Leichsenring et al., 2022; Leiblfinger et al., 2020). It was not just the border closures that evidenced such fault lines, but also the social isolation in which most personal carers and their clients (mostly over 80 years old) spend their everyday lives together. Those who were in the country during lockdowns worked under particularly precarious conditions for months, and those who were in their home country during that period had to persist without work and income. This situation made the precarious working conditions most visible – and even more:
Economically and ecologically, some critical questions also arise. From an ecological point of view, it is primarily about the carers’ long journeys across Europe. Economically, it is about (opportunity) costs and benefits from the different perspectives of those involved. Personal carers pay, after a short period of discount, the full social security contributions for self-employed. Overall, however, they only receive benefits of around 50% of the health insurance contributions paid (Rechnungshof Österreich, 2018). In contrast, public expenditures for subsidies amount to around 155 million euros yearly. These subsidies are received by 75% of all clients (the main aim of this subsidy had originally been to cover the additional costs incurred through compulsory social insurance). In any case, these expenditures are negligible if compared to the overall savings that Austria can record through the personal carers – without them, at least 20,000 more places in nursing homes and/or other care alternatives in the community would be needed. Even the approximately 1.5 billion euros that are currently flowing out of Austria per year, primarily to Romania and Slovakia, would not suffice to cover such an investment. Not to mention the fact that already the existing care homes and service providers cannot find trained nursing staff so that entire units remain closed. Thousands of additional relatives would have to consider how they could balance their employment with caring for their loved ones, and many would possibly (have to) give up their jobs and become full-time informal carers.
At the end of 2023, there were 57,634 self-employed personal carers still registered with the Chamber of Commerce, but the number has been declining since 2019. There is also a decline in the number of subsidies granted – only around 22,000 applicants received them at the end of 2023, while at the same time the number of those entitled to long-term care allowance had increased to 476,228 (+3.7%). The subsidy for personal carers had been increased for the first time in 2023 by 16.6% to 800 euros per month in order to eventually compensate for the most recent waves of inflation. A further increase of this subsidy as well as an increase in the income limit, which should also enable access for people with an income of over 2,500 euros, was claimed by the Chamber of Commerce and most recently also by a new platform of patient, relatives, staff and provider representatives (www.wko.at).
Money alone will not solve the fundamental problem areas of the 24-hour care model. As in so many industries, and especially in long-term care in general, the shortage of labour is becoming the greatest challenge.
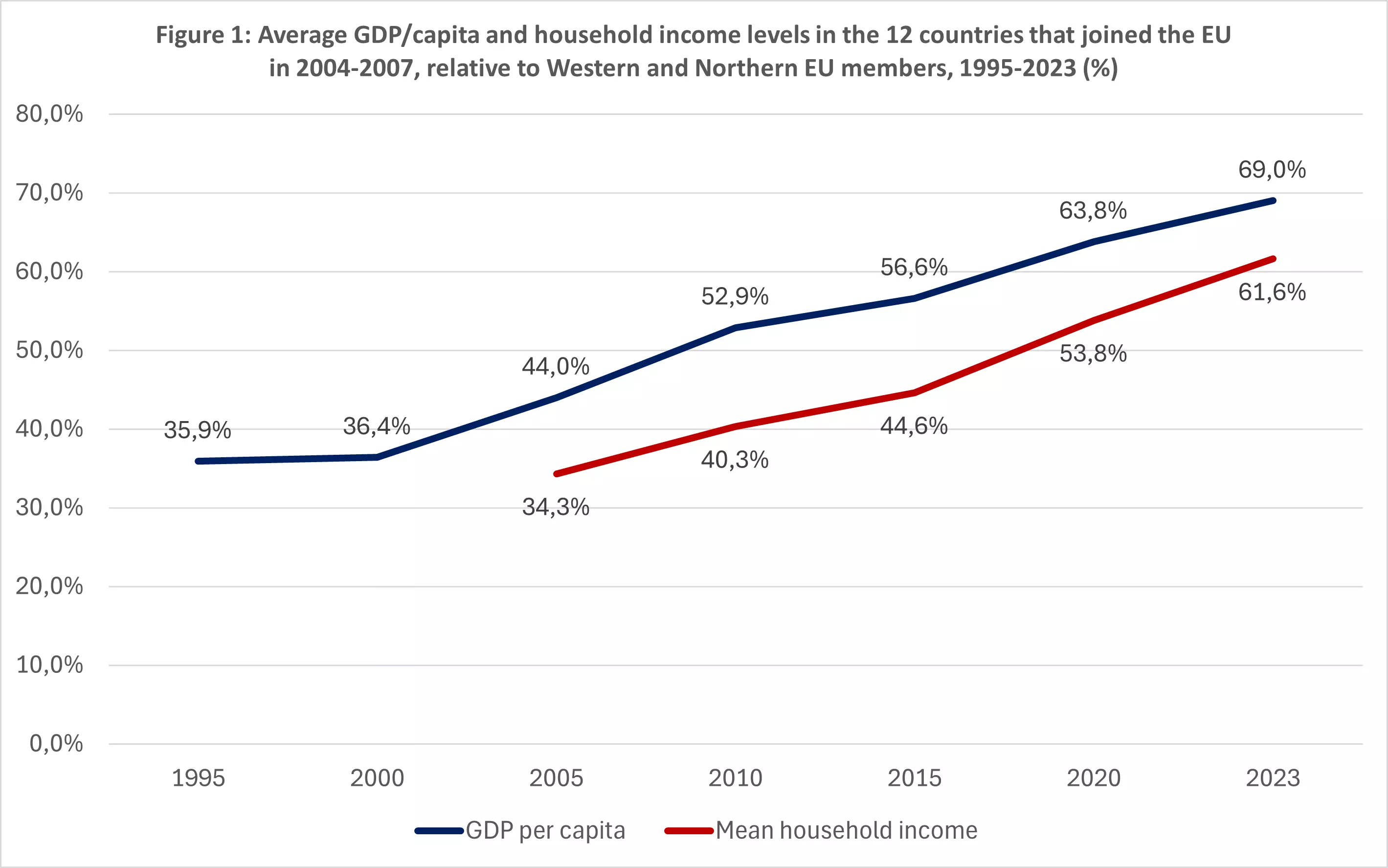
24-hour care will not disappear overnight in Austria, but the way Eastern European Member States have caught up with the richest EU countries has been impressive since 2004. While 20 years ago household incomes in the new EU Member States in the middle-income range reached just 25% of the richest EU countries, today this figure is around 62% (Darvas, 2024, see Figure 1). In Slovakia, only 25% of health and nursing staff earn less than 2,000 euros – self-employed personal carers in Austria are rarely paid more.
It is therefore high time to prepare for a steady decline of migrant personal carers from Eastern Europe and for taking appropriate precautions. Austria could still learn a lot from experiences in countries where the model of 24-hour care usually only causes people to shake their heads – in Sweden, Norway or even the Netherlands, this form of care is viewed as inadmissible exploitation, or at least legally as bogus self-employment. Although there is a model of personal assistance for people with disabilities in the Netherlands (in fully paid employment with clear rules against bogus self-employment), there is otherwise a well-developed network of social services and care homes based on long-term care insurance. However, the issue of staff shortages is also on the agenda in the Netherlands, because the high proportion of nursing staff in total employment includes an above-average percentage of employees who work part-time.
In Switzerland, too, personal care in private households is only possible as part of an employment relationship with the respective protection stipulated by labour law. In Spain and Italy, important legal reforms and collective bargaining agreements have been implemented in recent years, but undeclared work in households still plays an immensely important role.
How might Ljiljana be doing now? Like many of her colleagues, she is now near retirement age, her daughter has completed her studies and her parents will increasingly be confronted with age-related health problems. She herself will find the regular travel days more of a burden, but above all the increasingly demanding care tasks for her clients. The attempt by the Austrian federal government to index family allowances in 2018 will have offended her at least as much as how 24-hour carers were treated during the pandemic (Leichsenring et al., 2022). If she is still working as a personal carer, she has probably joined the ‘Iniciativa24: Representing the interests of Slovakian 24-hour carers’ at the latest during the Corona crisis. This initiative later joined forces with the ‘DREPT’ (Justice in Nursing and Personal Care) initiative, launched by Romanian carers, and eventually united in the IG24. At the same time, a separate group developed within vidaflex that claims to be Europe’s first trade union initiative for one-person entrepreneurs. It has now positioned itself as the largest voluntary advocacy group for 24-hour carers in Austria. vidaflex is also about combating bogus self-employment and enforcing workers’ rights, for example when agencies lead carers to believe that they are actually employed. Together with carers, vidaflex has developed a platform that brokers independent 24-hour carers. The aim is to position vidaflex as a ‘better’ placement agency and to use the platform to organise adequately trained carers through a direct contract between the carer and the person being cared for. vidaflex and IG24 thus represent the concerns of carers with one voice. Specifically, it is about the fight against bogus self-employment, addressing the grey area between care and nursing, but also (sexual) violence in the workplace, in order to regain overall dignity as women and migrant workers.
A future scenario could be to create something like collective bargaining in the area of 24-hour care, as was recently suggested in the 2024 social report by the Federal Ministry of Social Affairs, Health, Care and Consumer Protection (BMSGPK, 2024). This would require a significant reorganisation on the part of the employers – the placement agencies already organised in the Chamber of Commerce would be one possibility if they became real employers. Another option could be the foundation of an association of employing families such as, for instance, in Italy.
It is doubtful whether Ljiljana’s active colleagues will experience real collective bargaining negotiations or even an employment relationship as personal carers during their working lives. What is certain is that questions of one-person companies, platform work and bogus self-employment will continue to be our concern in policy and research during times of demographic and technological transformation in the world of work – including lucky findings, but in particular a further development towards more integrated long-term care systems.